Abstract
The disaster preparedness of community health nurses plays a crucial role in their ability to perform effectively during crises. This study assessed the level of disaster preparedness among community health nurses in the 5th District of Camarines Sur, focusing on their knowledge, skills, communication, and resources, as well as the intrinsic and extrinsic factors influencing their preparedness. A descriptive-correlational research design was utilized involving 102 community health nurses. Data were collected using a survey questionnaire and analyzed through percentage, weighted mean, and chi-square test. Findings revealed that majority of respondents were aged 31 - 40 years, female, married, bachelor’s degree holders, with 6 - 10 years of service, and had attended disaster-related training. In terms of preparedness, respondents are knowledgeable, moderately skilled, and agree to have communication competencies. In addition, resources were found to be quite sufficient, indicating existing limitations in logistical and material support. Intrinsic and extrinsic factors were found to often influence disaster preparedness. Statistical analysis showed that age, educational attainment, and length of service were not significantly related to preparedness, along with knowledge. However, sex, civil status, and attendance in disaster preparedness training were significantly related. Training was also significantly associated with skills and communication, while no significant relationship was found between profile variables and resources, suggesting that resource availability is largely influenced by institutional support. The study concludes that while community health nurses demonstrate preparedness in knowledge, skills, and communication, improvements in resource allocation and continuous training are necessary. A proposed enhancement plan was developed to address identified gaps through structured training programs, improved resource management, and strengthened organizational support to further enhance disaster preparedness among community health nurses.
Keywords
Disaster preparedness Community health nurses Intrinsic factors Extrinsic factors Disaster training.
Introduction
Natural disasters, and sadly disasters wrought by malice, remain a reality to many people in the world, including the Philippines. A country that is related to flooding or earthquakes, to name just two examples, risks devastation of community infrastructure. Community health nurses are invaluable in providing needed nursing care to families who may be confused and frightened. It could be a matter of life and death whether these nurses are ready to provide good quality health care in case of emergencies like these. Preparedness for emergencies means taking a coordinated approach, from identifying hazards, to assessing risk, designing an emergency response plan and building frontline responder capability.
Disaster preparedness at the community level allows stakeholders to respond quickly and appropriately within their own contexts. Community health nurses can help mitigate disasters, engage in health education, communicate early warnings, and respond in an emergency, and they are vital facilitators in disaster prevention and recovery (World Health Organization, 2021). Effective preparedness can lessen the negative impacts of disasters and speed up recovery; it requires coordinated collaboration between government and health agencies and local stakeholders. In particular, as described by the United Nations, building local capacity is the foundation of sustainable disaster risk reduction and resilience (UNDRR, 2022). Around the world, disaster preparedness has become an indispensable aspect of disaster risk management (DRM) owing to the growing threat posed by natural and human-made hazards. “Earthquakes, typhoons, pandemics, and climate-related events remind us why we need preparedness,” as stated by Goniewicz et al. (2023).
Disaster preparedness encompasses diverse strategies, such as early warning systems, standardized training courses, drills and run-throughs, and other efforts to enhance public awareness to improve the effectiveness of disaster response and minimize adverse impacts on health and society (Goniewicz et al., 2023). The Sendai Framework for Disaster Risk Reduction 2015–2030 is global policy to reduce disaster risks in all countries and all sectors. The Sendai Framework is structured along four priority areas: understand disaster risk; strengthen disaster risk governance; invest in disaster risk reduction for resilience; and disaster preparedness for effective response. At the national level, Republic Act No. 10121, otherwise known as the Philippine Disaster Risk Reduction and Management Act of 2010, was enacted due to the fragile nature of the country, making it highly susceptible to experiencing an increasing occurrence and intensity of disasters. RA 10121 marked a shift from the previously reactive, response-oriented framework established by Presidential Decree 1566 to a more strategic approach encompassing prevention, preparedness, response, and recovery.
The law created the National Disaster Risk Reduction and Management Council (NDRRMC) and directed the setting up of Local Disaster Risk Reduction and Management Offices (LDRRMOs) at various levels of government. It prioritizes community involvement, capacity development, and the incorporation of disaster risk reduction in local development planning. This is bolstered by the National Disaster Risk Reduction and Management Plan (NDRRMP) 2020-2030, which emphasizes resilience-building, climate change adaptation, and a whole-of-society approach towards disaster risk management. The new framework stresses the significance of proactive, risk-informed methods while reinforcing the significance of local government units and community partners in driving forward disaster preparedness and response (National Disaster Risk Reduction and Management Council, 2020).
The Fifth District of (Baao, Balatan, Bato, Buhi, Bula, Nabua, City of Iriga), Camarines Sur is located in a very dangerous area of the Bicol Region having the strong possibility of wilting hydro-meteorological hazards being located within the Bicol River floodplain and the being exposed to weather from the Pacific (Mines and Geosciences Bureau Region V, 2022). These geographic and climatic characteristics make communities more vulnerable to recurring flooding and other disaster-related weather effects on public health services and emergency response capacity. Studies show that municipalities in the Fifth District have varying degrees of exposure to disasters such as flooding, landslides, and typhoon hazards that affect communities and local infrastructure (Almelor et al., 2024). These hazards require heightened disaster preparedness of particularly community health nurses, who will primarily be responders to these emergencies in accordance with national disaster preparedness (National Disaster Risk Reduction and Management Council, 2020). The researcher, having been one of the community health nurses assigned in Buhi, Camarines Sur, a municipality prone to natural disasters and having dealt with the pains and agony of handling the disaster without full knowledge, skills, communication, and resources, is in a unique position to conduct this study on the disaster preparedness of community health nurses. Being familiar with the problems in the field, the study will assess the level of preparedness of the community health nurses. And by knowing where the community health nurses needed to be improved upon, the present study being done will serve as a basis to enhance and strengthen the disaster preparedness of our community health nurses.
Methodology
The study utilized a descriptive correlational research design to determine the level of disaster preparedness of the community health nurses in the Fifth District of Camarines Sur. This geographically and socioeconomically diverse locale includes the municipalities of Bato, Balatan, Nabua, Baao, Bula, Buhi, and Iriga City. Using the total enumeration sampling technique, the researcher targeted all community health nurses of the RHUs (Rural Health Units) and the City Health Office (CHO), resulting in a final sample of 102 respondents following the exclusion of respondents from Nabua and Bula.
Data collection was facilitated through a structured, self-administered instrument formulated in alignment with the objectives of the study. The questionnaire consisted of sections covering the respondents’ profile and key variables including knowledge, skills, communication, resources, and factors affecting disaster preparedness, categorized into intrinsic and extrinsic factors. The instrument underwent a validation process that included an initial draft presented to an oral examination panel and a pilot study using it with ten nurses and midwives to measure clarity and relevance, resulting in an acceptable reliability with a Cronbach’s alpha coefficient of 0.95. The validated questionnaires were disseminated in printed format or through online survey platforms like Google forms while ensuring the confidentiality of answers.
For the statistical treatment of data, the researcher systematically employed the percentage technique to determine the profile of the respondents and the weighted mean to assess levels of preparedness and affecting factors. A Four-point Likert Scale was utilized to quantify subjective data, with range values interpreted from “Highly Prepared” to “Not at all”. Additionally, the Chi-square test of independence was used to determine the significant relationship between the demographic profile and disaster preparedness among the community health nurses. This statistical analysis helped in identifying trends, patterns, and significant relationships to arrive at a fuller understanding of the nurses' preparedness.
Results and Discussion
Profile of the Respondents
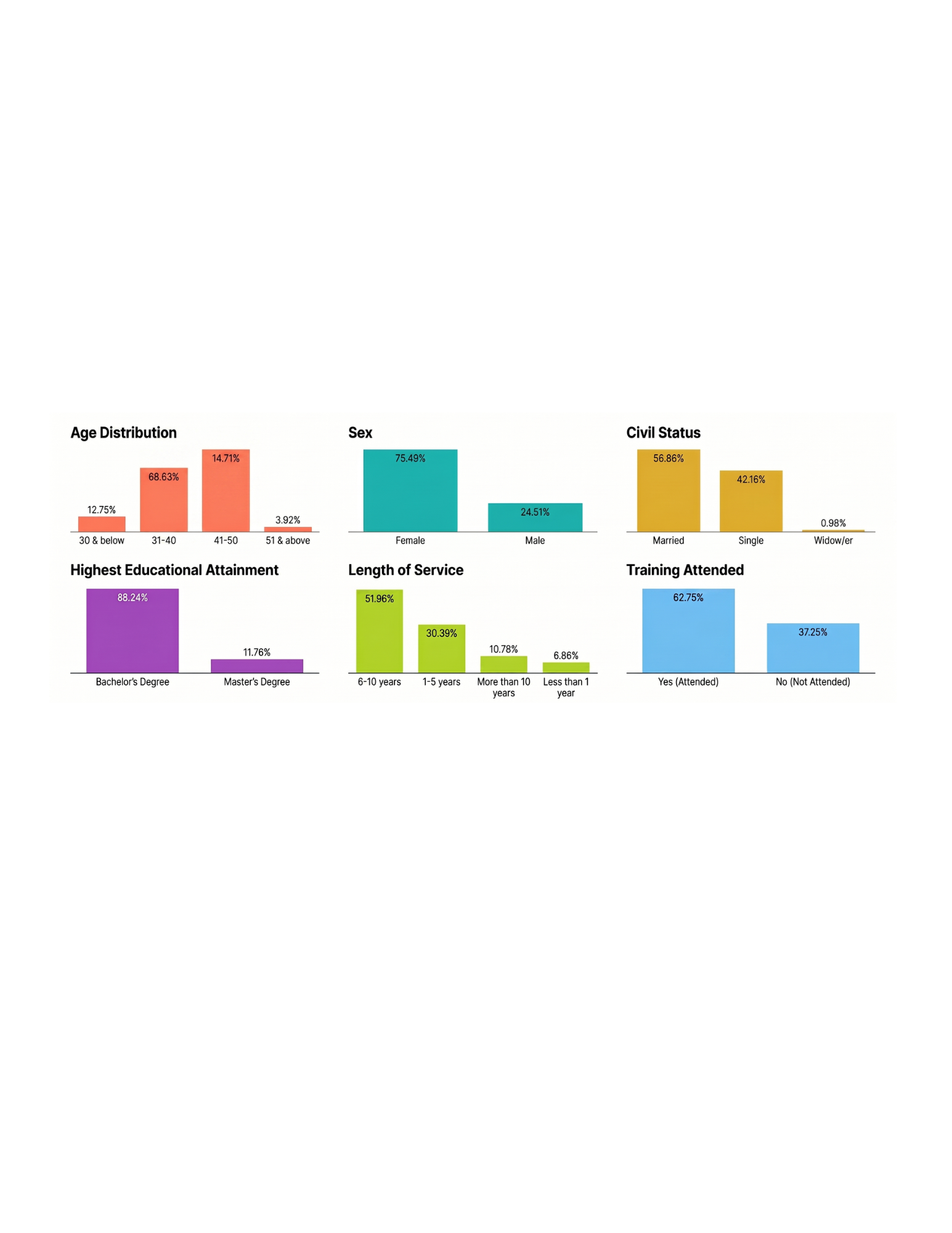
As presented in Figure 1, the 102 community health nurses were within the 31 to 40 age group (68.63%), making them the most represented group. This was followed by those aged 41 to 50 years with 15 respondents (14.71%), those aged 30 years and below with 13 (12.75%), and only 4 respondents (3.92%) aged 51 and above. In terms of sex, the group was predominantly female, 77 respondents (75.49%), while males made up 25 (24.51%). Majority of the respondents were married (58; 56.86%), followed closely by single individuals (43; 42.16%), and only one respondent (0.98%) was widowed. Regarding educational attainment, the majority held a bachelor’s degree (90; 88.24%), while a smaller portion had earned a master’s degree (12; 11.76%).
In terms of professional experience, more than half of the respondents had been in service for 6 to 10 years (53; 51.96%), indicating moderate experience. This was followed by those with 1 to 5 years of service (31; 30.39%), more than 10 years (11; 10.78%), and less than 1 year (7; 6.86%). When it comes to disaster preparedness training, 64 respondents (62.75%) reported having attended relevant training, while 38 (37.25%) had not. Overall, the respondents are predominantly female, mid-career nurses with bachelor’s degrees, many of whom have some exposure to disaster preparedness training, although a notable portion still lacks such training.
Level of Disaster Preparedness Among Community Health Nurses in the Fifth District of Camarines Sur
Knowledge. The overall level of knowledge of community health nurses in the fifth district of Camarines Sur in disaster preparedness was assessed to be prepared, as shown in Table 1. Consequently, knowledge of the types of disasters (natural, man-made, and biological), an indication that got the highest rating with a weighted mean of 3.42, next is the sense of their roles and responsibilities during disaster, with a weighted mean of 23. Knowledge of the different phases of disaster management, mitigation, preparedness, response, and recovery is obtained beyond the scaled score of 3.13, followed in order by the proper use of emergency equipment with a weighted mean of 3.12. The least is the familiarization with the Incident Command System (ICS), with a weighted mean of 2.99. Overall, a mean weighted score of 3.18 is presented and interpreted as “prepared.” Basically, community health nurses have fair knowledge as to the concepts of disaster and disaster management and their responsibilities in their profession in emergencies.
| Indicators | Weighted Mean | Verbal Interpretation |
| 1. Understands the different types of disasters (natural, man-made, and biological) that can affect the community. | 3.42 | Prepared |
| 3. Identifies the roles and responsibilities to be performed during a disaster. | 3.23 | Prepared |
| 2. Knowledgeable about the phases of disaster management (mitigation, preparedness, response, recovery). | 3.13 | Prepared |
| 5. Knowledgeable about the proper use of emergency equipment and supplies. | 3.12 | Prepared |
| 4. Familiar with the Incident Command System (ICS) applied during emergencies. | 2.99 | Prepared |
| Average Weighted Mean | 3.18 | Prepared |
Skills. The level of preparedness of community health nurses in the fifth district of Camarines Sur in terms of skills related to disaster preparedness. Of the indicators, the highest-ranked skill was the ability to recognize and prioritize vulnerable groups in the community that may require more assistance during disasters, with a weighted mean of 3.25. This was followed by the skill of contributing to the formulation of community disaster preparedness plans, which got the next highest weighted mean of 3.13. Capability of working in disaster situations under pressure garnered a weighted mean of 3.11. Providing first aid (physical and psychological) and basic life support, infection prevention and control garnered the lowest weighted means of 3.10. Overall, an average weighted mean of 3.14, interpreted as “Prepared.” It shows that the respondents have a fair level of proficiency in skills related to disaster preparedness but still need enhancement to achieve a higher level. The findings suggest that community health nurses have relative strengths in recognizing and prioritizing vulnerable populations that are key to sound needs-based disaster response.
| Indicators | Weighted Mean | Verbal Interpretation |
| 3. Identify and prioritize vulnerable groups needing special assistance during disasters | 3.25 | Prepared |
| 1. Can contribute to the development of community disaster preparedness plans. | 3.13 | Prepared |
| 2. Capable of working effectively in a high-pressure disaster situation. | 3.11 | Prepared |
| 4. Skilled in providing first aid (physical and psychological) and basic life support to disaster victims. | 3.10 | Prepared |
| 5. Can implement infection prevention and control measures in disaster settings. | 3.10 | Prepared |
| Average Weighted Mean | 3.14 | Prepared |
Communication. The level of preparedness of community health nurses in the fifth district of Camarines Sur in terms of communication skills during disasters. Among the indicators, having access to current emergency contact information for key response teams ranked highest, with a weighted mean of 3.36. This was followed by the ability to document and report events effectively, which obtained a weighted mean of 3.30. Confidence in communicating with diverse populations garnered a weighted mean of 3.25. Meanwhile, the ability to provide accurate and timely public information received a weighted mean of 3.21, and understanding the use of communication tools such as radios and hotlines recorded the lowest weighted mean of 3.16.
Overall, the average weighted mean of 3.25 was interpreted as “Prepared” which suggests that the respondents feel moderately prepared in communicating during disaster. It appears that the community health nurses do demonstrate communication preparedness during disaster, as indicated by the competencies of maintaining updates of contact systems and proper documentation and reporting. These are vital competencies, necessary for proper coordination and communication, timely decision-making, and continuity of care during a disaster. The aspect, however, generally scored lower, suggesting that communication tools and dissemination of public information need to be trained and enhanced. Areas for improvement could include these and other aspects using simulation exercises and communication drills and training on emergency communication technology.
| Indicators | Weighted Mean | Verbal Interpretation |
| 1. Has access to current emergency contact information for key response teams. | 3.36 | Prepared |
| 5. Can document and report events effectively during and after a disaster. | 3.30 | Prepared |
| 4. Feels confident in communicating with people from diverse backgrounds during emergencies. | 3.25 | Prepared |
| 2. Can provide accurate and timely information to the public during a disaster. | 3.21 | Prepared |
| 3. Understands how to use available communication tools (e.g., radios, hotlines, apps) during emergencies. | 3.16 | Prepared |
| Average Weighted Mean | 3.25 | Prepared |
Resources. Availability of resources by respondents in the fifth district of Camarines Sur. Availability of evacuation sites and emergency shelters in the community signified the highest or strongly bare-out resources with a weighted mean of 3.36. Next were those of transportation and mobility, with a weighted mean of 2.96, which implied the availability of transport and evacuation resources. Supplies, such as first aid and medicines with a weighted mean of 2.85 and guidelines and checklists with a weighted mean of 2.85, also turn out to be available typed-out items, which received the least, with a weighted mean of 2.75. The overall average weighted mean stood at 2.95 to be interpreted as "prepared." This study indicates that although there are robust physical assets available to support evacuation sites and shelters, many other key logistical or protective items that affect the safety and well-being of frontline health care providers during disaster responses have significant gaps.
The lower rating of PPE available for the frontline worker suggests potential issues with respect to their safety and protection during disaster responses. In addition, the moderately low level of access to medical supplies and transportation resources indicates a need for better resource allocation and overall system strengthening as well as improved logistical planning.
| Indicators | Weighted Mean | Verbal Interpretation |
| 5. The community has designated evacuation sites and emergency shelters. | 3.36 | Prepared |
| 4. Transportation and mobility resources are available for emergency response and evacuation. | 2.96 | Prepared |
| 2. The facility has supplies (e.g., first aid, medications) for disaster response. | 2.85 | Prepared |
| 3. Guidelines and checklists for disaster response are available. | 2.85 | Prepared |
| 1. Personal protective equipment (PPE) during disaster situations. | 2.75 | Prepared |
| Average Weighted Mean | 2.95 | Prepared |
Factors Affecting the Disaster Preparedness of Community Health Nurses in the Fifth District of Camarines Sur
Intrinsic Factors. Table 5 presents the influence of intrinsic factors on the disaster preparedness of community health nurses in the Fifth District of Camarines Sur. Among the indicators, “I am motivated to enhance knowledge and skills in disaster preparedness”, obtained the highest weighted mean of 3.48. This was followed by “I am personally committed to disaster preparedness as part of my nursing role”. with a weighted mean of 3.46, and “I remain motivated to serve the community despite difficult circumstances” with a weighted mean of 3.39. Self-discipline in following emergency procedures and safety protocols garnered a weighted mean of 3.37, while being proactive in seeking information about disaster risks and safety measures received a weighted mean of 3.34. “I stay updated on health risks and trends related to disasters”, obtained a weighted mean of 3.31. Meanwhile, “I feel confident in my ability to make decisions during disaster situations” and “I am emotionally prepared to respond to emergencies”, both recorded weighted means of 3.28. The lowest-ranked indicators are “I take the initiative to participate in disaster-related training or simulations., and “I believe I can lead others during a disaster if needed”, both with weighted means of 3.24. Overall, the average weighted mean of 3.34, interpreted as “Affect,” indicating that intrinsic motivators such as personal commitment, motivation, confidence, and proactive behavior influence nurses’ disaster preparedness.
The results show that community health nurses have substantial internal resources that encourage them to be ready for emergency circumstances, especially in terms of motivation, commitment to the profession, and willingness to improve their competencies. The internal qualities that community health nurses demonstrate positively affect their participation in preparedness activities and adherence to safety standards; however, their lower ratings for training participation and leadership confidence show that intrinsic drivers don't always correlate with active participation in emergency preparedness and leadership.
| Indicators | Weighted Mean | Verbal Interpretation |
| 10. I am motivated to enhance knowledge and skills in disaster preparedness. | 3.48 | Affect |
| 1. I am personally committed to disaster preparedness as part of my nursing role. | 3.46 | Affect |
| 9. I remain motivated to serve the community despite difficult circumstances. | 3.39 | Affect |
| 6. Self-disciplined in following emergency procedures and safety protocols | 3.37 | Affect |
| 8. Proactive in seeking information about disaster risks and safety measures. | 3.34 | Affect |
| 7. I stay updated on health risks and trends related to disasters. | 3.31 | Affect |
| 2. I feel confident in my ability to make decisions during disaster situations. | 3.28 | Affect |
| 5. I am emotionally prepared to respond to emergencies. | 3.28 | Affect |
| 3. I take the initiative to participate in disaster-related training or simulations. | 3.24 | Affect |
| 4. I believe I can lead others during a disaster if needed. | 3.24 | Affect |
| Average Weighted Mean | 3.34 | Affect |
Extrinsic Factors. The influence of extrinsic factors on the disaster preparedness of community health nurses in the Fifth District of Camarines Sur. Table 6 presents that among the indicators, the existence of a local disaster risk reduction plan within the facility ranked highest, with a weighted mean of 3.50. This was followed by coordination between local government agencies and health personnel, which obtained a weighted mean of 3.46, and the geographical risk characteristics of their assigned work areas, with a weighted mean of 3.33. The presence of clear policies defining disaster response roles garnered a weighted mean of 3.32, while support and guidance from supervisors received a weighted mean of 3.23. Sufficient personnel to share responsibilities obtained a weighted mean of 3.10.
`Meanwhile, structural safety of health facilities and accessibility of evacuation centers both recorded weighted means of 3.09. The lowest-ranked indicators were disaster drills and simulation exercises (3.00) and regular evaluations of preparedness levels (2.96). In summary, nurses’ disaster preparedness is significantly impacted by external, environmental, and organizational variables with an average weighted mean of 3.20, interpreted as Affect.
It can be inferred that having formalized systems and formalized guidelines
positively impact nurses’ disaster preparedness and support toward preparing for these events. In addition, structural support components, such as leadership and adequate staff, also help nurses to be ready for addressing disaster events. The exercise drills, simulations, and regular assessment ratings of disaster training have comparatively lower evaluations.
This suggests that there is a lack of practical application and ongoing assessment of disaster readiness. For safety and evacuation access to be modestly rated indicates a need for improvement in the physical infrastructure and resources. With routine training, systematic assessment, and the commitment of resources to the health care system for resilient health facilities, these components will improve overall disaster readiness. Additionally, having a preparedness culture will help elevate the level of proactive involvement of nurses in disaster-related responsibilities from their respective institutions. Therefore, continuous capacity-building efforts for health care institutions will help maintain the level of readiness and adaptive capacity for new disaster risks.
| Indicators | Weighted Mean | Verbal Interpretation |
| 1. The facility has an existing local disaster risk reduction plan. | 3.50 | Greatly affect |
| 3. Local government agencies coordinate effectively with health workers during disasters. | 3.46 | Affect |
| 5. The geographical location of my assigned area increases the risk of natural disasters. | 3.33 | Affect |
| 2. There are clear policies that define my role during disaster response. | 3.32 | Affect |
| 7. I receive strong support and guidance from supervisors during disasters. | 3.23 | Affect |
| 6. There are enough personnel to share responsibilities during a disaster. | 3.10 | Affect |
| 8. Health facilities are structurally safe and equipped to function during disasters. | 3.09 | Affect |
| 9. Evacuation centers and shelters in the community are accessible and properly equipped. | 3.09 | Affect |
| 4. Disaster drills and simulation exercises are regularly conducted. | 2.97 | Affect |
| 10. The facility conducts regular evaluations of our disaster preparedness level. | 2.96 | Affect |
| Average Weighted Mean | 3.20 | Affect |
Relationship Between the Profile of the Respondents and the Level of Preparedness of Community Health Nurses in the Fifth District of Camarines Sur
Relationship Between the Profile of the Respondents and the Level of Preparedness of Community Health Nurses Along with Knowledge. The relationships between selected profile variables of community health nurses in the Fifth District of Camarines Sur and their level of disaster preparedness in terms of knowledge is shown in Table 7. The analysis shows that age (p = 0.116), highest educational attainment (p = 0.944), and length of service (p = 0.443) were not significantly associated with disaster preparedness knowledge, as their p-values exceed the conventional threshold of 0.05. In contrast, sex (p = 0.001), civil status (p = 0.009), and attendance in disaster preparedness–related training (p = 0.012) demonstrated statistically significant relationships with preparedness in terms of knowledge. The practically significant relationships indicate that social and gender are more important factors, participation in disaster preparedness training, and levels of knowledge than age, education, or length of time in service. Participation in disaster preparedness training is particularly noteworthy. Attending training sessions enhanced nurses' knowledge related to disasters, highlighting that competency-based education in disaster preparedness is imperative.
These findings have dire implications for the nursing profession and programs of disaster preparedness. Broadly classified demographic factors of age, educational experience, and years of service are not going to predict disaster preparedness knowledge. Rather, active and structured participation, equitable opportunities, and social or gender involvement are essential to preparedness. Disaster preparedness, being made accessible to all community health nurses and having the approach individualized, enhances overall knowledge and awareness of disasters.
| Indicators | Computed X2-Value | p-value @ 0.05 | Decision on Ho | Interpretation |
| Age | 10.2 | 0.116 | Accepted | Not Significant |
| Sex | 13.3 | 0.001 | Rejected | Significant |
| Civil Status | 13.4 | 0.009 | Rejected | Significant |
| Highest Educational Attainment | 0.16 | 0.944 | Accepted | Not Significant |
| Length of Service | 5.83 | 0.443 | Accepted | Not Significant |
| Attended Training Related to Disaster Preparedness | 8.81 | 0.012 | Rejected | Significant |
Relationship Between the Profile of the Respondents and the Level of Preparedness of Community Health Nurses Along with Skills. The analysis examining the relationship between selected demographic and professional profile variables and the level of disaster preparedness among community health nurses in the Fifth District of Camarines Sur in terms of skills is illustrated in Table 8. As indicated by the results, however, most of the personal and professional data of the respondents, such as age (p = 0.576), sex (p = 0.082), civil status (p = 0.446), highest educational attainment (p = 0.690), and length of service (p = 0.489), are not significantly associated with disaster preparedness skills. Of the variables studied, only attendance in disaster preparedness‐related training was found to be significantly associated with skills (p = 0.005).
It can be gathered that nurses who are trained in disaster and formal disaster training programs perceived themselves as more ready and competent on the response to such disaster as their training highlights the skill‐based preparedness. These findings indicate that variables such as age, sex, civil status, level of education, and years of work experience alone cannot predict level of skill competency in disaster preparedness. On the other hand, practical skill competencies improve, emphasizing targeted education that includes hands-on experiences. Use of simulation exercises, scenario-based drills, and competency assessments will allow the nurse to be not only knowledgeable but competent and directed to effective disaster response.
| Indicators | Computed X2 -Value | p-value @ 0.05 | Decision on Ho | Interpretation |
| Age | 4.75 | 0.576 | Accepted | Not Significant |
| Sex | 5.00 | 0.082 | Accepted | Not Significant |
| Civil Status | 3.71 | 0.446 | Accepted | Not Significant |
| Highest Educational Attainment | 0.74 | 0.690 | Accepted | Not Significant |
| Length of Service | 5.44 | 0.489 | Accepted | Not Significant |
| Attended Training Related to Disaster Preparedness | 10.6 | 0.005 | Rejected | Significant |
Relationship Between the Profile of the Respondents and the Level of Preparedness of Community Health Nurses Along with Communication. Table 9 presents the results of tests examining the relationships between selected profile variables and the level of disaster preparedness of community health nurses in the Fifth District of Camarines Sur in terms of communication. Communication is a critical component of disaster preparedness, encompassing information dissemination, coordination, and teamwork during emergencies. Age (p = 0.124), civil status (p = 0.377), highest educational attainment (p = 0.803), and length of service (p = 0.693) did not show any significant relationship with communication disaster preparedness. Sex (p = 0.001) and attendance for disaster preparedness-related training (p = 0.015) were the variables significantly related to communication skills, but attendance for disaster communication preparedness training significantly contributed to their higher communication preparedness skills based on the main results of this study. Targeted training plays a central role in developing communication competencies. Enhancing communication skills through structured training programs, including modules on risk communication, interprofessional collaboration, and community engagement, can strengthen nurses’ ability to coordinate effectively, share critical information, and engage stakeholders during emergencies.
| Indicators | Computed X2 -Value | p-value @ 0.05 | Decision on Ho | Interpretation |
| Age | 10.0 | 0.124 | Accepted | Not Significant |
| Sex | 14.7 | 0.001 | Rejected | Significant |
| Civil Status | 4.22 | 0.377 | Accepted | Not Significant |
| Highest Educational Attainment | 0.44 | 0.803 | Accepted | Not Significant |
| Length of Service | 3.88 | 0.693 | Accepted | Not Significant |
| Attended Training Related to Disaster Preparedness | 8.36 | 0.015 | Rejected | Significant |
Relationship Between the Profile of the Respondents and the Level of Preparedness of Community Health Nurses Along with Resources. Table 10 presents the relationships between selected profile variables and the level of disaster preparedness of community health nurses in the Fifth District of Camarines Sur in terms of resources. The analysis reveals that none of the variables including age (p = 0.795), sex (p = 0.904), civil status (p = 0.927), highest educational attainment (p = 0.962), length of service (p = 0.891), and attendance in disaster preparedness training (p = 0.071) were significantly associated with preparedness in terms of resources, as all p-values exceeded the conventional 0.05 level of significance. Thus, relationships between professional characteristics of nurses and their perceptions of the availability and adequacy of resources for response to disasters were not found. This implies that resource-related preparedness is largely independent of individual profiles and instead influenced by other considerations. Specifically, community health nurses seem to need background activities in resource development and management rather than individual characteristics to enhance their preparedness. Availability and actual efficacy of resources appear to be institutionally dependent on the support of structured training programs, facilities, and emergency planning.
| Indicators | Computed X2 -Value | p-value @ 0.05 | Decision on Ho | Interpretation |
| Age | 5.44 | 0.795 | Accepted | Not Significant |
| Sex | 0.57 | 0.904 | Accepted | Not Significant |
| Civil Status | 1.92 | 0.927 | Accepted | Not Significant |
| Highest Educational Attainment | 0.29 | 0.962 | Accepted | Not Significant |
| Length of Service | 2.00 | 0.891 | Accepted | Not Significant |
| Attended Training Related to Disaster Preparedness | 7.02 | 0.071 | Accepted | Not Significant |
Proposed Plan to Enhance the Disaster Preparedness of Community Health Nurses in the Fifth District of Camarines Sur
The aim of the plan is to address specific disaster preparedness gaps as well as knowledge, skills, communication, resources, and factors affecting disaster preparedness (intrinsic and extrinsic), while harnessing individual and organizational factors to improve the readiness of nurses to respond in disaster situations. By outlining areas of concern, specific objectives, activities, responsible personnel, and expected outcomes, the plan provides a structured approach to improving the disaster preparedness of nurses within the community health setting.
Rationale
Disasters, both natural and man-made, can endanger an at-risk community. Community health nurses are on the frontline of the disaster and must ensure continuity of care and timely interventions. They must protect the health and safety of those involved in disasters. Research has suggested that they may not have the training to do this effectively, and this proposed health plan is needed. The proposed plan aims to instill competence, confidence, and readiness in community health nurses to provide efficient, well-coordinated, equitable care to the communities they serve during disasters.
General Objective
To enhance the disaster preparedness of community health nurses by strengthening their knowledge, skills, communication, and resources, while addressing the intrinsic and extrinsic factors that affect their disaster preparedness, thereby improving their overall capacity to respond effectively and efficiently during disaster situations.
Table 12. Proposed Plan to Enhance the Disaster Preparedness of Community Health Nurses in the Fifth District of Camarines Sur
| Areas of Concern | Specific Objectives | Activities/ Strategies | Persons Involved | Expected Outcomes |
| 1. Disaster Preparedness a. Resources Personal protective equipment (PPE) during disaster situations | To ensure sufficient supply and equitable distribution of PPE during emergencies. To establish proper inventory and stockpiling systems for PPE. To ensure occupational safety and infection control compliance. | Conduct needs assessment and inventory of existing PPE supplies. Develop a PPE stockpiling and replenishment plan at the municipal level. Coordinate with local government units for logistics and supply chain management | Municipal Health Officer Nurse Supervisors Local Government Unit (LGU) Officials DRRM Officers Supply/Logistics Officers Community Health Nurses | Improved availability and timely distribution of PPE during disasters. Strengthened compliance with health and safety standards. Reduced occupational exposure and infection risks among nurses |
| b. Skills Skilled in providing first aid (physical and psychological) and basic life support to disaster victims Can implement infection prevention and control measures in disaster settings c. Knowledge d. Communication Understands how to use available communication tools (e.g., radios, hotlines, apps) during emergencies 2. Factors Affecting a. Extrinsic Factors The facility conducts regular evaluations of our disaster preparedness level b. Intrinsic Factors I take the initiative to participate in disaster-related training or simulations I believe I can lead others during a disaster if needed | To enhance practical skills in physical first aid and emergency trauma care. To strengthen competence in delivering Psychological First Aid (PFA) to affected individuals. To build confidence in responding to real-life disaster scenarios. To enhance knowledge and practical skills in infection prevention and control during disasters. To improve the capability in preventing outbreaks in evacuation centers and affected communities. To ensure compliance with national IPC protocols. To enhance nurses’ understanding of the structure, roles, and functions of ICS. To enhance practical skills and strengthen adherence to proper communication protocols and the chain of command To improve coordination and timely reporting during disaster response. To establish a routine system for evaluating disaster preparedness at the facility level. To identify strengths and gaps in disaster response readiness To align facility practices with national disaster preparedness standards To enhance leadership and self-confidence during disaster-related training. To strengthen decision-making and crisis management skills. To develop leadership competencies aligned with disaster response structures. To cultivate a pool of nurse leaders in emergency situations. | Organize certified BLS and CPR training sessions with return demonstrations. Facilitate Psychological First Aid (PFA) seminars and role-playing activities. Implement simulation-based drills. Conduct periodic refresher courses and competency assessments. Conduct Infection prevention and control training workshops focused on disaster contexts. Demonstrate proper PPE donning and doffing, and waste disposal procedures. Organize simulation exercises involving outbreak scenarios. Develop and distribute quick-reference Infection prevention and control guidelines for disaster response. Conduct regular monitoring and evaluation of Infection and prevention control. Conduct orientation-seminars on ICS concepts and organizational structure. Provide training workshops on role delegation, chain of command, and communication flow under ICS. Organize tabletop exercises and simulation drills applying ICS scenarios (e.g., typhoon, flood, earthquake). Distribute simplified ICS manuals and quick-reference guides Conduct orientation on local emergency communication systems and reporting protocols. Facilitate simulation drills incorporating communication breakdown scenarios. Develop a standardized evaluation checklist based on NDRRMC and DOH guidelines. Conduct scheduled drills and tabletop exercises with post-assessment reviews. Hold feedback sessions and Integrate evaluation results into facility planning and training schedules. Conduct leadership and crisis management workshops focused on disaster scenarios. Facilitate scenario-based drills where nurses rotate as team leaders. Implement mentorship programs pairing experienced nurses with emerging leaders. Provide feedback and reflective debriefing sessions after simulations. | Municipal Health Officers Nurse Supervisors Licensed BLS/CPR Trainers (e.g., accredited trainers from the Philippine Red Cross) DRRM Officers Mental Health Professionals / Psychologists Community Health Nurses Municipal Health Officers Nurse Supervisors Trained DOH Infection Control Personnel DRRM Officers Sanitary Inspectors Community Health Nurses Municipal Health Officer Nurse Supervisors Trainers from the Disaster Risk Reduction and Management (DRRM) office. Community Health Nurses Municipal Health Officer Nurse Supervisors Local DRRM Officers IT/Communications Personnel from DRRM Community Health Nurses Municipal Health Office Nurse Supervisors DRRM Officers Community Health Nurses Municipal Health Officers Nurse Supervisors DRRM Officers Leadership/Disaster Management Trainers Community Health Nurses | Improved technical competence in first aid and BLS procedures. Increased ability to provide immediate psychological support to disaster victims. Standardized emergency care practices among community health nurses. Enhanced confidence and readiness in managing emergency situations. Improved adherence to infection prevention and control standards during disasters. Reduced risk of communicable disease outbreaks. Increased confidence of nurses in managing public health risks. Strengthened coordination between health and sanitation teams. Enhanced community safety and protection during disaster response. Increased knowledge and understanding of ICS principles among community health nurses. Improved coordination and role clarity during disaster response. Enhanced confidence in functioning within structured emergency management systems. Strengthened alignment of nursing response with national disaster protocols. Improved technical competence and confidence in operating communication tools during emergencies. Faster and more accurate reporting of incidents and health concerns. Strengthened inter-agency coordination during disaster. Improved frequency and quality of disaster preparedness evaluations. Identification and timely addressing of preparedness gaps. Increased accountability and adherence to protocols. Enhanced organizational readiness for real disaster events Increased confidence in assuming leadership roles during disasters. Improved coordination and decision-making during emergency response. Enhanced teamwork and delegation skills. Development of competent nurse leaders. |
Conclusions
The following were the conclusions derived from the study: It was found that the majority of the respondents were aged between 31 to 40 years, female, and married. Most of the respondents graduated with a Bachelor’s degree, had 6 to 10 years of service and attended training on disaster preparedness. Community health nurses have a sound understanding of the types of disasters, such as natural, manmade, and biological, that can occur in the community. Community health nurses can identify the special groups who will need assistance during a disaster. Having an emergency contact list in hand ensures that communication will be made with the appropriate teams if and when needed. The presence of designated evacuation sites and emergency shelters within the community indicates that essential measures for disaster preparedness are in place. Community health nurses expressed interest in learning and practicing disaster preparedness, while the presence of a disaster risk reduction plan in place at the facility suggested that systems are available to assist when required.
Not all profile variables were significantly associated with the level of disaster preparedness of community health nurses. Knowledge, age, highest educational attainment, and length of service showed no significant relationship. However, sex, civil status, and attendance in disaster preparedness–related training were found to have significant relationships with knowledge. Attendance in disaster preparedness–related training was found to have a significant relationship with the level of preparedness of community health nurses in terms of skills. The findings revealed that age, civil status, highest educational attainment, and length of service were not significantly related to the level of preparedness of community health nurses in terms of communication. However, sex and attendance in disaster preparedness–related training showed significant relationships. None of the profile variables were significantly related to the level of preparedness of community health nurses in terms of resources.
The proposed plan aims to address gaps in disaster preparedness among community health nurses in terms of knowledge, skills, communication, and resources, as well as the intrinsic and extrinsic factors influencing preparedness. It adopts both individual and organizational strategies to strengthen nurses’ capacity to effectively respond to disaster situations by identifying key concerns, setting objectives, outlining appropriate activities, designating responsible personnel, and defining expected outcomes.
Recommendations
Based on the conclusions of the study, the following are being recommended:
1. Brigade development programs for nurses of all ages, underscoring that disaster preparedness trainings may be made available to every community health nurse in the realm.
2. Continue and improve regular education and awareness programs about the types of disasters to keep nurses with a solid basic understanding that will be useful for disaster preparedness. Develop guidelines and modules about how to identify vulnerable groups during disasters and how to respond to them so that our nurses can provide targeted and timely support. Ensure that all community health nurses have updated and ready access to emergency contact lists for the various teams they are coordinating with, and make this part of drills. Work with barangays in getting to know evacuation sites and shelters, and pilot with sites on how they expect things to work.
3. Encourage attendance at continuing education sessions, workshops, and professional development opportunities as a way to keep nurses engaged and involved in disaster preparedness and disaster risk reduction planning. Integrate nurses’ roles into the facility’s disaster risk reduction plan so that they know the processes to follow, what roles and responsibilities they will play, and what protocols to put in place during emergencies.
4. Advocate for disaster preparedness training for all nurses. Evidence suggests that attendance in such workshops, simulations, and drills significantly increases knowledge in disaster response regardless of age, education, or number of years in service. Advocate for disaster training programs that teach skills. Unless programs include practice with assessing resources before a disaster or practical activities on being better prepared, then programs can be an ineffective use of time. Advocate for communication training so that nurses can know how to communicate with those responding to a disaster, internally coordinating information, and reporting information that could save lives.
5. Adopt and implement the proposed disaster preparedness plan using both individual and organizational approach strategies, delineating roles and responsibilities, and evaluate outcomes that improve nurses’ overall disaster response capacity.
References
- Almelor, M. T., Villanueva, P. M. B., Bayos, G. B., & Orbita, D. (2024). Disaster risk reduction and management policies and programs of the municipalities in the Fifth District of Camarines Sur: A comprehensive analysis. Polaris Global Journal of Scholarly Research and Trends, 3(4), 1–22. DOI ↗ Google Scholar ↗
- Goniewicz, K., Khorram-Manesh, A., Burkle, F. M., Hertelendy, A. J., Goniewicz, M., & Jakubczak, R. (2023). The role of preparedness in disaster risk reduction: Strategies for effective response and resilience. International Journal of Environmental Research and Public Health, 20(4), 3210. DOI ↗ Google Scholar ↗
- Mines and Geosciences Bureau Region V. (2022). Geohazard assessment and flood susceptibility maps of Camarines Sur. Department of Environment and Natural Resources. DOI ↗ Google Scholar ↗
- National Disaster Risk Reduction and Management Council. (2020). National disaster risk reduction and management plan (2020–2030). NDRRMC. DOI ↗ Google Scholar ↗
- National Disaster Risk Reduction and Management Council. (2024). National Disaster Risk Reduction and Management Plan 2024–2030. DOI ↗ Google Scholar ↗
- United Nations Office for Disaster Risk Reduction. (2022). Global assessment report on disaster risk reduction 2022: Our world at risk—Transforming governance for a resilient future. UNDRR. DOI ↗ Google Scholar ↗
- World Health Organization. (2021). Strengthening health emergency preparedness and response in communities: WHO guidance. World Health Organization. DOI ↗ Google Scholar ↗